
Levels of serum albumin peak at about 20 years old (~4.6 g/dL for males, ~4.4 g/dL for females), then decrease during aging, as shown for the 1,079,193 adults of Weaving et al. (2016):
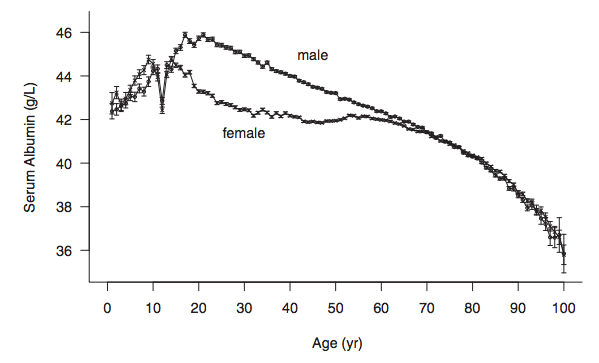
Similar age-related decreases for serum albumin albumin have also been reported in smaller studies: Gom et al. 2007 (62,854 subjects); Dong et al. 2010 (2,364 subjects); Le Couteur et al. 2010 (1,673 subjects); Dong et al. 2012 (1,489 subjects).
Why is it important that serum levels of albumin decrease during aging? Reduced levels of albumin are associated with an increased risk of death from all causes. For example, in the 1,704,566 adults of Fulks et al. 2010, serum albumin levels > 4.4 g/dL and 4.5 g/dL for females and males, respectively, were associated with maximally reduced risk of death from all causes, regardless of age (younger than 50y, 50-69y, or 70y+):

The association between reduced levels of serum albumin with an increased risk of death from all causes have also been found in smaller studies. In a ~9 year study of 7,735 men (age range, 40-59y), when serum albumin was less than 4 g/dL, the mortality rate was 23/1000/per year, compared with 4/1000/per year for subjects with values greater than 4.8 g/dL (Phillips et al. 1989):
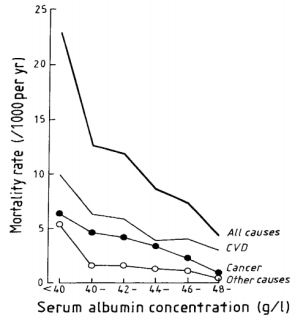
Similarly, in older adults (average age, ~80y, 672 subjects), serum albumin levels greater than 4.5 g/dL (equivalent to 45 g/L) were associated with significantly reduced all-cause mortality risk, when compared with compared with < 4.1 g/dL (equivalent to 41 g/L, Takata et al. 2010):

Decreased levels of serum albumin (less than 4 g/dL) being associated with an increased all-cause mortality risk was also identified in a 12-year study of 287 older adults (average age, ~75y, Sahyoun et al. 1996).
Can the age-related decrease in serum albumin be minimized, or prevented? Shown below is my data for serum albumin since 2005, when I was 32y:
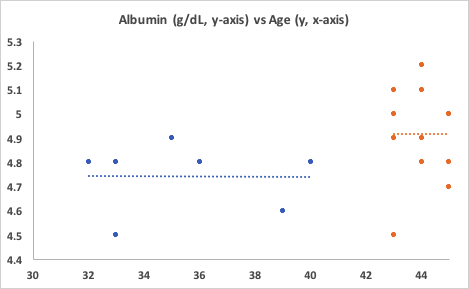
First, note the period from when I was 32y until 40y. No age-related decrease! My average albumin value over 7 measurements was 4.74 g/dL. Unfortunately, I didn’t track my dietary info during that time.
Also note the period from 43y to 45y. First, my albumin levels are significantly higher than the first period, 4.92 g/dL (p=0.027)! Second, again note the absence of an age-related decrease. Based on the data of Weaving et al. (2016), my albumin levels should be around 4.4 g/dL, but I’ve got them going in the opposite direction! How have I been able to do that?
Since April 2015, with use of a food scale, I’ve been tracking my daily dietary intake, including macro and micronutrients (54 variables). For each orange data point in the second period, I have an average dietary intake for each of the 54 variables that I can use to correlate with serum albumin. Based on that data, I can make an educated guess at what could potentially increase, or decrease it.
Of the 54 dietary variables that I track, only 3 were significantly correlated with albumin: positive associations for alpha-carotene (r = 0.66, p = 0.027), beta-carotene (r = 0.75, p =0.007), and a negative association for Vitamin K (r = -0.64, p = 0.03). Shown below is the strongest correlation of the three, beta-carotene, vs. serum albumin.
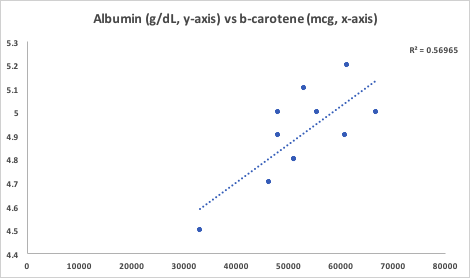
The majority of my alpha and beta-carotene intake comes from carrots, with a smaller amount coming from butternut squash. Interestingly, beta-cryptoxanthin, a Vitamin A metabolite that is abundant in butternut squash, was not significantly associated with serum albumin. Butternut squash is also a good source of alpha- and beta-carotene, so if butternut squash was driving the correlation between the carotenes with albumin, I’d expect beta-crypoxanthin to also be significantly associated with it. However, since it’s not, carrots are the most likely source driving the association. Also note that the my average intake of Vitamin K is dramatically higher (1410 mcg; range, 1080-2203 mcg) than the RDA or AI, which are ~100-120 mcg/day. The negative association between my Vitamin K intake with albumin suggests that I should keep it closer to 1100 mcg/day to potentially keep my albumin levels high.
If you’re interested, please have a look at my book!
References
Dong MH, Bettencourt R, Barrett-Connor E, Loomba R. Alanine aminotransferase decreases with age: the Rancho Bernardo Study. PLoS One. 2010 Dec 8;5(12):e14254.
Dong MH, Bettencourt R, Brenner DA, Barrett-Connor E, Loomba R. Serum levels of alanine aminotransferase decrease with age in longitudinal analysis. Clin Gastroenterol Hepatol. 2012 Mar;10(3):285-90.e1.
Gom I, Fukushima H, Shiraki M, Miwa Y, Ando T, Takai K, Moriwaki H. Relationship between serum albumin level and aging in community-dwelling self-supported elderly population. J Nutr Sci Vitaminol (Tokyo). 2007 Feb;53(1):37-42.
Dong MH, Bettencourt R, Barrett-Connor E, Loomba R. Alanine aminotransferase decreases with age: the Rancho Bernardo Study. PLoS One. 2010 Dec 8;5(12):e14254.
Fulks M, Stout RL, Dolan VF. Albumin and all-cause mortality risk in insurance applicants. J Insur Med. 2010;42(1):11-7.
Le Couteur DG, Blyth FM, Creasey HM, Handelsman DJ, Naganathan V, Sambrook PN, Seibel MJ, Waite LM, Cumming RG. The association of alanine transaminase with aging, frailty, and mortality. J Gerontol A Biol Sci Med Sci. 2010 Jul;65(7):712-7.
Phillips A, Shaper AG, Whincup PH. Association between serum albumin and mortality from cardiovascular disease, cancer, and other causes. Lancet. 1989 Dec 16;2(8677):1434-6.
Sahyoun NR, Jacques PF, Dallal G, Russell RM. Use of albumin as a predictor of mortality in community dwelling and institutionalized elderly populations. J Clin Epidemiol. 1996 Sep;49(9):981-8.
Takata Y, Ansai T, Soh I, Awano S, Sonoki K, Akifusa S, Kagiyama S, Hamasaki T, Torisu T, Yoshida A, Nakamichi I, Takehara T. Serum albumin levels as an independent predictor of 4-year mortality in a community-dwelling 80-year-old population. Aging Clin Exp Res. 2010 Feb;22(1):31-5.
Weaving G, Batstone GF, Jones RG. Age and sex variation in serum albumin concentration: an observational study. Ann Clin Biochem. 2016 Jan;53(Pt 1):106-11.

My 44-year-old wife has an albumin level of 51 and an albumin/globulin ratio of nearly 2:1. People usually think she’s 35 or younger.
BTW you’ve told me to remind you that you’d promised a new “What I eat” post…;-)
LikeLike
Those are great numbers, Zoltan! The key is to identify which dietary/supplements/exercise regimen are best correlated with them, so that she can maintain them for as long as possible!
LikeLike
My own albumin level is 48, up from 46 last year, which is very good news. The albumin:globulin ratio nevertheless decreased from 1.7:1 to 1.65:1 as my globulin level went from 27 to 29 – but I don’t think I should be concerned about that.
LikeLike
Good news on the albumin, Zoltan. It decreases with age, and lower levels are associated with increased all-cause mortality risk, so it’s important to make sure that it stays high. The globulin value, though, is going in the wrong direction. Values ~2.2-2.5 may be optimal… Interestingly, elevated globulin may be related to seasonality: my globulins are consistently within that range, by I suffer from allergies (grass) every June, and as of last week were 3.6! So I’m definitely keeping an eye on them, to make sure they’re not still elevated once the allergies pass.
LikeLike
Oh yes, I have the same seasonal pollen allergy (grass, in June).
LikeLike
Do you take anything to lessen the symptoms? I don’t, I just suffer each June through a relatively clogged nose and itchy eyes…Interestingly, I’ve had my blood measured for 3 consecutive June’s, and I see a pattern of 3x elevated eosinophils. I have tracked dietary data, too, so in a couple of years I’ll have a lot of data to try dietary interventions.
LikeLike
Pingback: Optimizing Serum Levels Of Albumin: Data From 20 Blood Tests – Michael Lustgarten
Pingback: Biohacking for Tummies: How Your Vanity Can Increase Your Longevity | Bottom Line Inc
This is awesome…a possible way to raise my albumin test results! Albumin is my worst lab value, and wondering what i might do to improve it is what brought me to this wonderful site, with so many more topics of interest. Eating more carrots sounds to me like a sure-bet proposition: it may or may not raise my albumin, but I doubt I could bring myself to eat enough to hurt me. I’m just not sure about the timing.
Before reading these posts of Dr. Lustgarten, I had come across a couple of small studies using oral and IV L-Carnitine to raise albumin levels in some fairly sick patients. Here’s the one which used 250g of L-Carnitine orally 3 times/day: https://www.researchgate.net/publication/256474332_The_Effect_of_Oral_L-carnitine_on_Serum_Albumin_and_Inflammatory_Markers_Levels_in_Patients_under_Peritoneal_Dialysis_A_Randomized_Controlled_Trial. Has anyone else seen or tried this? Or did it not seem worthwhile? Anyway, ahead of my next lab tests, I had already started taking the L-Carnitine to see if I could make the albumin figure budge..
Now, if I take both and one works, I won’t know which one it was that worked. So I think I should keep on with the L-Carnitine until I see the results of that intervention. Then, only after my next lab tests, I should switch to carrots and see what effect I can discern from them.
Will report on results either way. Meanwhile any comments or suggestions welcome.
LikeLike
Good luck, and keep me posted on the carnitine supplementation. What happens if it increases albumin, but makes other markers worse? Finding which approach is best for all the markers, not just 1 is important.
LikeLike
Did you have any markers in mind to watch out for? From my reading I understand excess carnitine is generally excreted, but here is some cardiac risk from excess carnitine via TMAO produced by gut microbiota (which spp?) in meat eaters (such as myself). But I have no idea where this would show up in any test, let alone what might mediate that effect.
AFAIK I am at low risk for CAD (high HDL, low TG, low CRP), but I bear in mind I am already supplementing with ALCAR 500-1000mg/day, on top of about .8g/kg animal protein/day.. I do walk (or dance) the equivalent of 8 miles a day most days (plus occasional weights & sports), so I estimate I probably need more protein than most women my age. Does that sound reasonable?
LikeLike
Should be .4g/kg animal protein, not .8!
LikeLike
Mine’s 4.9/5.0! With A/G ratio of 2.3 and 1.8!
LikeLike
That’s great, Alex. The key (obviously) keep it there for many decades!
LikeLike