
In an earlier post I wrote about the association between elevated circulating levels of homocysteine with an increased risk of death from all causes (https://michaellustgarten.wordpress.com/2017/11/22/homocysteine-and-all-cause-mortality-risk/). I started to post updates in that link, but I’ve decided to move them to here.
As of 6/2018, I now have tracked dietary data (I weigh all my food and record the values in cronometer.com) that corresponds to 7 homocysteine measurements:
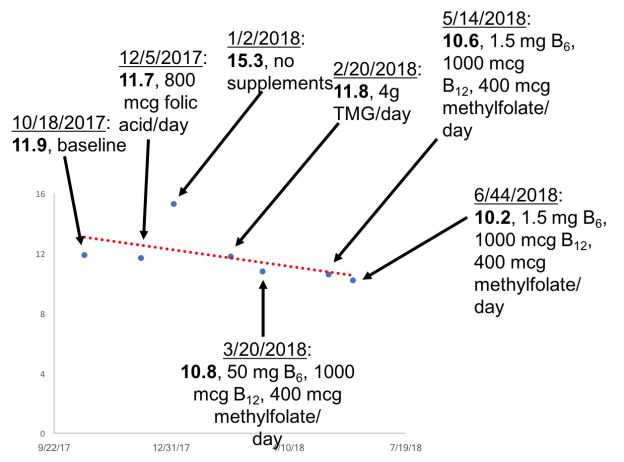
12/5/2017: Despite 42 days of 800 micrograms of supplemental folic acid, bringing my average daily folate intake to 2026 micrograms/day, my plasma homocysteine was essentially unchanged at 11.7 uMoL, when compared with my baseline value of 11.8 uMol.What’s next on the list to reduce it? Trimethylglycine, also known as betaine. I’m a proponent of using diet as a first strategy, and to increase my dietary betaine levels, I’ll eat beets and quinoa, bringing my daily betaine levels to ~500 mg/day. Let’s see how it turns out on my next blood test!
1/2/2018: ~500 mg/day of betaine from beets and quinoa did absolutely nothing to my homecysteine levels. In fact, it got worse (15.3 uMoL)! To test the hypothesis that it wasn’t enough betaine, next I tried 4 grams/day of betaine (also known as trimethylglycine, TMG).
2/20/18: Supplemental TMG did absolutely nothing in terms of reducing my homocysteine to values below baseline! Also note that there is evidence that TMG increases blood lipids, including LDL and triglycerides (TG; Olthof et al. 2005), and that’s exactly what it did to me. My average LDL and TG values since 2015 (11 measurements) are 77 and 50 mg/dL, respectively. On TMG, these values increased to 92 and 72 mg/dL, respectively, making them my highest values over 11 individual blood tests (with the exception of 1 day with an LDL of 93 mg/dL). Next, I tried a stack that included 50 mg of B6, 1000 mcg of B12, and 400 mcg of methylfolate, as supplementation with these B-vitamins has been shown to lower homocystine (Lewerin et al. 2003).
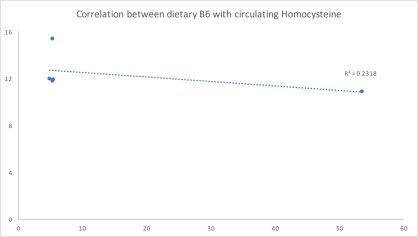
3/20/18: Finally, some progress! My homocysteine levels were reduced during the B-vitamin supplementation period. I’ve written it like that because I’m not sure if it was the B-vitamins that caused it. For example, in the image below, we see the correlation between my dietary B6 intake with homocysteine. The trendline is down, which I would expect if B6 supplementation actually is playing a role in reducing my homocysteine levels. However, note that the correlation between my dietary B6 levels with homocysteine is not very strong (r = .48), resulting in a moderate R2 of 0.23 (similar data was obtained for B12 and folate). With 5 blood test measurements corresponding to 5 dietary periods, if B6 is playing a role, I would expect a stronger correlation. Nonetheless, with more data, the correlation may strengthen, so stay tuned for that!
5/14/2018: I changed B6-B12-methylfolate supplements so that I’d only have to take pills from 1 bottle instead of from 3. That supplement, however, had 1.5 mg of B6 instead of the 50 mg that was in my original supplement. Less B6 didn’t result in a higher homocysteine value-in fact, it went down (slightly), from 10.8 to 10.6. If an increased amount of B6 was causing lower levels of homocysteine, I would’ve expected higher, not (barely) lower homocysteine levels. This suggests that maybe my B6 intake has nothing to do with my homocysteine levels.
6/4/2018: Despite no changes to my supplements, my homocysteine came down a little more, to 10.2. Interestingly, the correlation (r) between homocysteine with my total dietary (diet + supplements) intake of B6, B12, and methylfolate is 0.39, 0.68, 0.29, respectively. The correlation between my B12 intake with homocysteine looks moderately strong, whereas the correlations for B6 and folate are weak. Based on this data, it’s possible I had a mild B12 deficiency that was causing elevated homocysteine. Note that my average B12 intake, without supplements is ~8 mcg/day, which is more than 3-fold higher than the RDA.
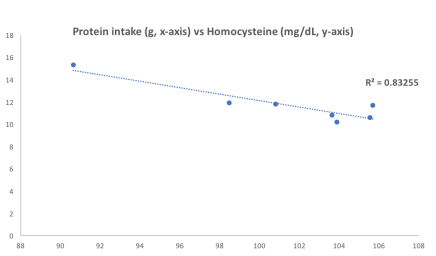
In looking at the association between my dietary data with homocysteine, a stronger correlation (r = 0.91; R2 = 0.83) has emerged…for my protein intake! In other words, a higher protein intake is more strongly correlated with lower homocysteine than B12:
7/11/2018: To explore the strong association between my protein intake with homocysteine, I increased my protein intake from an average value of 104 g/day for the period that preceded my June measurement (5/15/2018 – 6/4/2018) to 136 g/day for the period up to my 7/11/2018 measurement (6/5/2018 – 7/10/2018). The result? Lower homocysteine, to 8.2 uMol/L! Interestingly, the correlation between my dietary protein intake with homocysteine remained strong (r = 0.86, R2 = 0.73, n = 7 measurements).
What about my B6, methyl-B12, methyl-folate stack? I’m still taking it, although it looks like methyl-B12 may be the only factor that is associated with my homocysteine levels. In support of that, the correlation between each with homocysteine is r = 0.02, 0.73, 0.36, respectively.
Because I now have my homocysteine < 9 umol/L, it may be time to optimize other variables (in addition to the metabolic panel and CBC). Stay tuned!
If you’re interested, please have a look at my book:
References
Lewerin C, Nilsson-Ehle H, Matousek M, Lindstedt G, Steen B. Reduction of plasma homocysteine and serum methylmalonate concentrations in apparently healthy elderly subjects after treatment with folic acid, vitamin B12 and vitamin B6: a randomised trial.vEur J Clin Nutr. 2003 Nov;57(11):1426-36.
Olthof MR, van Vliet T, Verhoef P, Zock PL, Katan MB. Effect of homocysteine-lowering nutrients on blood lipids: results from four randomised, placebo-controlled studies in healthy humans. PLoS Med. 2005 May;2(5):e135.
