
On a recent blood test, my plasma level of homocysteine (Hcy) was 11.9 uMol. Is that optimal minimizing disease risk and maximizing longevity? Let’s have a look at the literature.
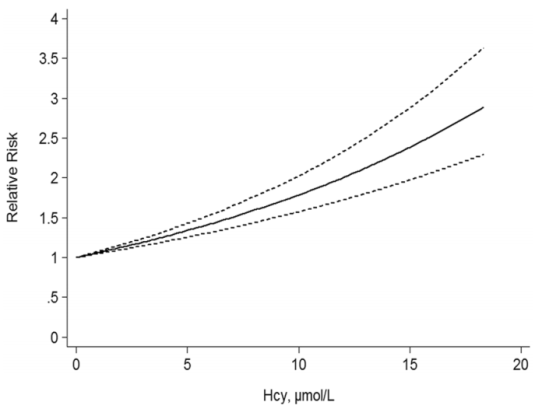
A 2017 meta-analysis of 11 studies including 27,737 participants showed an increased risk of death from all causes (“all-cause mortality”; ACM) as circulating levels of homocysteine increase (Fan et al. 2017):
When looking at meta-analyses, it’s important to examine each of the individual studies. Here are the data for the 11 included studies:
- Kark et al. 1999: 1,788 older adults, average age 65y, followed for 9-11 years. Compared with values less than 8.5 uMol, subjects with elevated homocysteine (> 14.7) had a 2-fold higher risk of death from all causes.
- Bostom et al. 1999: 1,933older adults, verage age, 70y, median follow-up, 10y. Subjects with values > 14.3 uMol had 2-fold ACM risk, when compared with < 14.3.
- Hoogeveen et al. 2000: 811 older adults (average age, 65y), 5 yr follow-up. Non- diabetics had a 34% increased ACM risk (p=0.08), but diabetics had 2.5-fold increased ACM risk after a 5-yr follow-up.
- Vollset et al. 2001: 4,766 older adults (age range, 65-67y at study entry), median 4 yr follow-up. Compared with 5.1-8.9 uMol, values greater than 12 were significantly associated with a 2.4-4.5 increased ACM risk.
- Acevedo et al. 2003. 3,427 subjects, average age 56y, ~3yr follow-up. ACM risk lowest for < 9.4 uMol, compared with > 14.4.
- González et al. 2007: 215 older adults (average age, 75y), median 4 yr follow-up. Compared with < 8.7 uMol, values > 16.7 had 2.3-fold increased ACM risk.
- Dangour et al. 2008: 853 older adults (average age, 79y), ~7.6y follow-up. Homocysteins > 19.4 uMol associated with ~2-fold higher ACM risk, when compared with < 9.8.
- Xiu et al. 2012: 1,412 older adults (average age, ~75y), up to 10 year follow-up. 1.8-fold higher ACM risk comparing those with >14.5 uMol with < 9.3.
- Waśkiewicz et al. 2012: 7,165 middle aged adults, ~5yr follow- up. 1.8-fold increased ACM risk for subjects with homocysteine > 10.5 uMol(average age, 52y) when compared with < 8.2 (avg age, 40y).
- Wong et al. 2013: 4,248 older men, average age ~77y, ~5yr follow-up. 1.5-fold increased ACM risk for homocysteine values > 15 uMol.
- Swart et al. 2012: 1,117 older adults (average age, 75y), up to a 7yr follow-up. In 543 men, homocysteine was not associated with ACM risk. In 574 women, 1.7 to 1.9-fold higher ACM risk when comparing > 12.7 and >15.6 vs < 10.3 uMol.
Not included in their analysis:
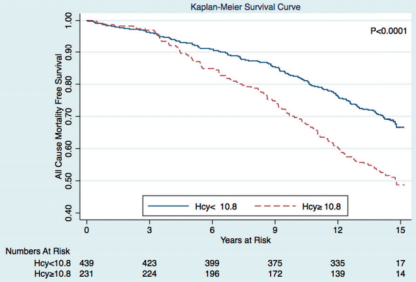
- Petersen et al. 2016: 670 subjects, average age 65y, average follow-up 14.5y. Subjects with homocysteine values ≥ 10.8 μmol/l had a significant higher incidence of all-cause mortality:
In sum, the evidence appears consistent across these 12 studies that elevated homocysteine is associated with an increased risk of death from all causes. Based on the Fan et al. (2016) meta-analysis, lower appears better, with values < 5 uMol associated with maximally reduced ACM risk. Also based on that data, my ACM risk is ~1.5-fold increased!
To see how dietary changes and supplements have impacted my homocysteine levels, see this link: https://michaellustgarten.wordpress.com/2018/03/23/reducing-homocysteine-updates/
If you’re interested, please have a look at my book:
References:
Bostom AG, Silbershatz H, Rosenberg IH, Selhub J, D’Agostino RB, Wolf PA, Jacques PF, Wilson PW. Nonfasting plasma total homocysteine levels and all-cause and cardiovascular disease mortality in elderly Framingham men and women. Arch Intern Med. 1999 May 24;159(10):1077-80.
Dangour AD, Breeze E, Clarke R, Shetty PS, Uauy R, Fletcher AE. Plasma homocysteine, but not folate or vitamin B-12, predicts mortalityin older people in the United Kingdom. J Nutr. 2008 Jun;138(6):1121-8.
Fan R, Zhang A, Zhong F. Association between Homocysteine Levels and All-cause Mortality: A Dose-Response Meta-Analysis of Prospective Studies. Sci Rep. 2017 Jul 6;7(1):4769.
González S, Huerta JM, Fernández S, Patterson AM, Lasheras C. Homocysteine increases the risk of mortality in elderly individuals. Br J Nutr. 2007 Jun;97(6):1138-43.
Hoogeveen EK, Kostense PJ, Jakobs C, Dekker JM, Nijpels G, Heine RJ, Bouter LM, Stehouwer CD. Hyperhomocysteinemia increases risk of death, especially in type 2 diabetes : 5-year follow-up of the Hoorn Study. Circulation. 2000 Apr 4;101(13):1506-11.
Kark JD, Selhub J, Adler B, Gofin J, Abramson JH, Friedman G, Rosenberg IH. Nonfasting plasma total homocysteine level and mortality in middle-aged and elderly men and women in Jerusalem. Ann Intern Med. 1999 Sep 7;131(5):321-30.
Petersen JF, Larsen BS, Sabbah M, Nielsen OW, Kumarathurai P, Sajadieh A. Long-term prognostic significance of homocysteine in middle-aged and elderly. Biomarkers. 2016 Sep;21(6):490-6.
Swart KM, van Schoor NM, Blom HJ, Smulders YM, Lips P. Homocysteine and the risk of nursing home admission and mortality in older persons. Eur J Clin Nutr. 2012 Feb;66(2):188-95.
Waśkiewicz A, Sygnowska E, Broda G. Homocysteine concentration and the risk of death in the adult Polish population. Kardiol Pol. 2012;70(9):897-902.
Wong YY, Almeida OP, McCaul KA, Yeap BB, Hankey GJ, Flicker L. Homocysteine, frailty, and all-cause mortality in older men: the health in men study. J Gerontol A Biol Sci Med Sci. 2013 May;68(5):590-8.
Vollset SE, Refsum H, Tverdal A, Nygård O, Nordrehaug JE, Tell GS, Ueland PM. Plasma total homocysteine and cardiovascular and noncardiovascular mortality: the Hordaland Homocysteine Study. Am J Clin Nutr. 2001 Jul;74(1):130-6.
