What are the blood biomarkers of a centenarian, and is there room for improvement? Find out in the video below!

Blood Test Analysis In A 100 Year Old Subject
Leave a reply
What are the blood biomarkers of a centenarian, and is there room for improvement? Find out in the video below!
CD8+ T cells are a subset of lymphocytes that play a major role in antiviral defense (Kulinski et al. 2013). However, recently published evidence shows reduced levels of circulating CD8+ T cells in people infected with SARS-CoV-2 (Zheng et al. 2020, Wang et al. 2020; HC= healthy controls, NCP = patients with COVID-19 related pneumonia):

Immune enhancing treatments, including thymalfasin and immunoglobulin are being provided to SARS-COV-2 infected subjects with some success. For example, 37/55 (67%) subjects saw improvements for circulating CD8+ levels in Wang et al. 2020, but additionally, 18/55 subjects did not experience increased CD8+ counts:

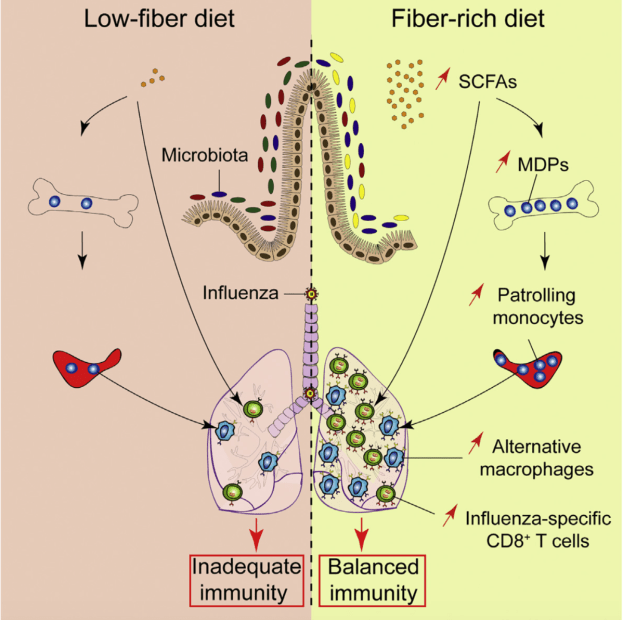
Accordingly, levels of CD8+ T cells were identified as an independent predictor for COVID-19 severity and treatment efficacy (Wang et al. 2020). When considering that CD8+ cells were not increased in all subjects in Wang et al., are there are other strategies that may be helpful? Interestingly, increased levels of CD8+ cells are found in the lungs of mice infected with the influenza A virus in response to a high soluble-fiber diet, when compared with control-fed mice (Trompette et al. 2018):

As a result, lung viral load is more than 10-times reduced 8-days after infection in high soluble fiber-fed mice:

Moreover, average survival in mice infected with influenza A is significantly better when fed the high soluble-fiber diet, when compared with control fed-mice:

Is it possible that a high soluble fiber diet can increase CD8+ cells in people infected with SARS-CoV-2, thereby enhancing their recovery and survival? No studies have tested this hypothesis (yet). While conventional medical treatment is obviously helpful, based on the findings of Trompette et al. (2018), further optimization of immune defense against viral infections may occur when including soluble fiber-rich foods.
References
Kulinski JM, Tarakanova VL, Verbsky J. Regulation of antiviral CD8 T-cell responses. Crit Rev Immunol. 2013;33(6):477-88. Review.
Trompette A, Gollwitzer ES, Pattaroni C, Lopez-Mejia IC, Riva E, Pernot J, Ubags N, Fajas L, Nicod LP, Marsland BJ. Dietary Fiber Confers Protection against Flu by Shaping Ly6c– Patrolling Monocyte Hematopoiesis and CD8+ T Cell Metabolism. Immunity. 2018 May 15;48(5):992-1005.e8. doi: 10.1016/j.immuni.2018.04.022.
Wang F, Nie J, Wang H, Zhao Q, Xiong Y, Deng L, Song S, Ma Z, Mo P, Zhang Y. Characteristics of peripheral lymphocyte subset alteration in COVID-19 pneumonia. J Infect Dis. 2020 Mar 30. pii: jiaa150. doi: 10.1093/infdis/jiaa150.
Zheng M, Gao Y, Wang G, Song G, Liu S, Sun D, Xu Y, Tian Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020 Mar 19. doi: 10.1038/s41423-020-0402-2.
Coronavirus isn’t the only virus that negatively affects human health.
For more info,
https://www.amazon.com/dp/B01G48A88A
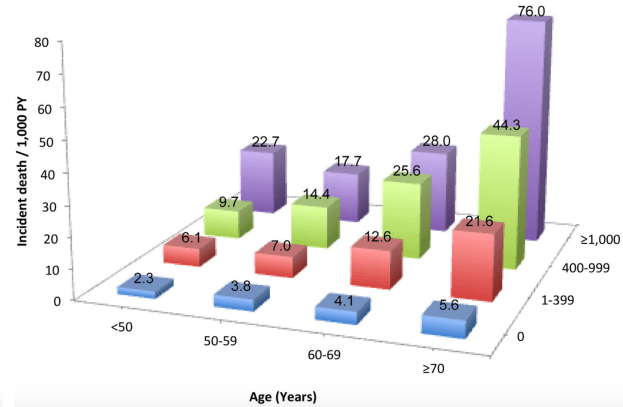
The coronary artery calcification (CAC) score is a measure of how much calcification is in the coronary arteries, and accordingly, is an in vivo measure of atherosclerosis. Why is the CAC score important? Besides its role in atherosclerosis, risk of death for all causes goes up at any age as the CAC score increases. For ex., in people younger than 50 (left side below), as the CAC score increases from 0 to 1-399, 400-999, and > 1000, risk of death for all causes increases by ~10-fold, from 2.3 per 1000 person years (PY) to 6.1/1000, 9.7/1000, and 22.7/1000. Similarly, for people older than 70y (right side below), as the CAC score increases, baseline all-cause mortality risk increases ~15-fold, from 5.6/1000 to 21.6/1000, 44.3/1000, and 76/1000, respectively (Hartaigh et al. 2016):

Are blood biomarkers associated with CAC? When the CAC score was elevated, a greater percentage of white blood cells (WBCs) that were neutrophils and the red blood cell distribution width (RDW%) were higher, whereas lower CAC scores were associated with higher levels for the fraction of lymphocytes divided by total WBCs and higher total red blood cells (den Harder et al. 2018):

In agreement with these data, CAC scores > 100 were associated with a higher RDW% (13.0%) and a higher neutrophil/lymphocyte ratio (NLR; 1.54), when compared with CAC < 100 (RDW = 12.8%; NLR = 1.39; Gürel et al. 2019).
The findings that a higher RDW% and higher levels of neutrophils, but lower levels of lymphocytes are associated with a higher CAC score is in agreement with the data for how these variables change with aging and their associations with all-cause mortality risk. First, note that I previously reported that RDW% increases during aging and is associated with an increased risk of death from all causes (https://michaellustgarten.wordpress.com/2019/09/25/optimizing-biological-age-rdw/). Similarly, neutrophils increase, whereas lymphocytes decrease, thereby leading to a higher neutrophil/lymphocyte ratio during aging, which is associated with an increased all-cause mortality risk (https://michaellustgarten.wordpress.com/2019/10/10/neutrophil-lymphocyte-ratio-and-survival/).
If you’re interested, please have a look at my book!
References
den Harder AM, de Jong PA, de Groot MCH, Wolterink JM, Budde RPJ, Iŝgum I, van Solinge WW, Ten Berg MJ, Lutgens E, Veldhuis WB, Haitjema S, Hoefer IE, Leiner T. Commonly available hematological biomarkers are associated with the extent of coronary calcifications. Atherosclerosis. 2018 Aug;275:166-173. doi: 10.1016/j.atherosclerosis.2018.06.017.
Gürel OM, Demircelik MB, Bilgic MA, Yilmaz H, Yilmaz OC, Cakmak M, Eryonucu B. Association between Red Blood Cell Distribution Width and Coronary Artery Calcification in Patients Undergoing 64-Multidetector Computed Tomography. Korean Circ J. 2015 Sep;45(5):372-7. doi: 10.4070/kcj.2015.45.5.372.
Hartaigh BÓ, Valenti V, Cho I, Schulman-Marcus J, Gransar H, Knapper J, Kelkar AA, Xie JX, Chang HJ, Shaw LJ, Callister TQ, Min JK. 15-Year prognostic utility of coronary artery calcium scoring for all-cause mortality in the elderly. Atherosclerosis. 2016 Mar;246:361-6. doi: 10.1016/j.atherosclerosis.2016.01.039.
In an earlier post, based on data from the Baltimore Longitidunal Study on Aging (BLSA), I suggested that total white blood cell (WBCs) counts between 3500 to 6000 cells per microliter of blood may be optimal for reducing disease risk and for maximizing longevity (https://michaellustgarten.wordpress.com/2015/08/13/blood-testing-whats-optimal-for-wbc-levels/).
However, within WBCs, neutrophils increase, whereas lymphocytes decrease during aging (Ruggiero et al. 2007, Starr and Dreary 2011). As a result, the ratio between neutrophils with lymphocytes (NLR) increases during aging from ~1.5 in 20 year olds to ~1.8 in adults older than 75y (Li et al. 2015):

An increased neutrophil/lymphocyte ratio during aging may be bad for health and disease risk. First, a higher neutrophil/lymphocyte ratio is associated with sarcopenia (defined as the age-related loss of muscle mass and physical function) in older adults (average age, 72y; Öztürk et al. 2018):

Second, risk of death for all causes is significantly increased for older adults (average age, 66y) that had higher NLR values (60-80%, >80%, equivalent to NLR = 1.92-2.41, > 2.41), when compared with lower NLR values (< 20%, 20-40%, 40-60%, equivalent to NLR < 1.90; Fest et al. 2019):

Similarly, all-cause mortality risk was 30% increased in older adults (average age, 54y) that had NLR values > 1.77, when compared with < 1.77, and 40% increased for NLR values > 2.15, when compared with < 2.15 (Kime et al. 2018).
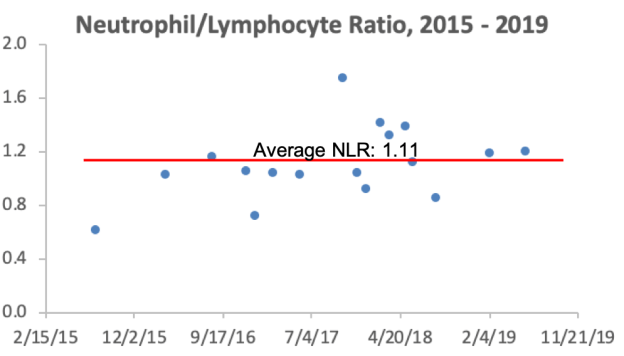
What are my NLR values? Over 17 blood test measurements from 2015 – 2019, my average NLR is 1.11. So far so good!

If you’re interested, please have a look at my book!
References
Fest J, Ruiter TR, Groot Koerkamp B, Rizopoulos D, Ikram MA, van Eijck CHJ, Stricker BH. The neutrophil-to-lymphocyte ratio is associated with mortality in the general population: The Rotterdam Study. Eur J Epidemiol. 2019 May;34(5):463-470.
Kim S, Eliot M, Koestler DC, Wu WC, Kelsey KT. Association of Neutrophil-to-Lymphocyte Ratio With Mortality and Cardiovascular Disease in the Jackson Heart Study and Modification by the Duffy Antigen Variant. JAMA Cardiol. 2018 Jun 1;3(6):455-462. doi: 10.1001/jamacardio.2018.1042.
Li J, Chen Q, Luo X, Hong J, Pan K, Lin X, Liu X, Zhou L, Wang H, Xu Y, Li H, Duan C. Neutrophil-to-Lymphocyte Ratio Positively Correlates to Age in Healthy Population. J Clin Lab Anal. 2015 Nov;29(6):437-43. doi: 10.1002/jcla.21791.
Öztürk ZA, Kul S, Türkbeyler İH, Sayıner ZA, Abiyev A. Is increased neutrophil lymphocyte ratio remarking the inflammation in sarcopenia? Exp Gerontol. 2018 Sep;110:223-229.
Ruggiero C, Metter EJ, Cherubini A, Maggio M, Sen R, Najjar SS, Windham GB, Ble A, Senin U, Ferrucci L. White blood cell count and mortality in the Baltimore Longitudinal Study of Aging. J Am Coll Cardiol. 2007 May 8;49(18):1841-50.
Starr JM, Deary IJ. Sex differences in blood cell counts in the Lothian Birth Cohort 1921 between 79 and 87 years. Maturitas. 2011 Aug;69(4):373-6.
