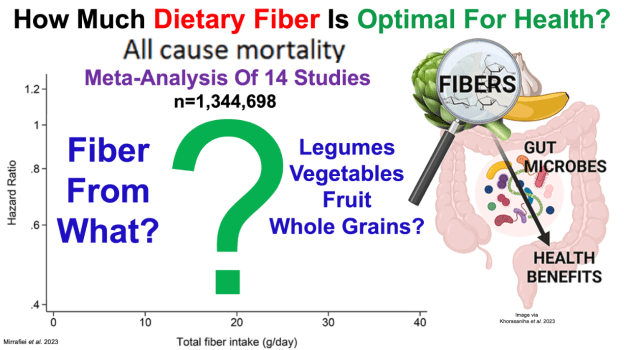
Papers referenced in the video: Total and different dietary fiber subtypes and the risk of all-cause, cardiovascular, and cancer mortality: a dose–response meta-analysis of prospective cohort studies https://pubmed.ncbi.nlm.nih.gov/37997693/
——————————————————————————————————————————-Paper referenced in the video: Tea consumption and attenuation of biological aging: a longitudinal analysis from two cohort studies https://pubmed.ncbi.nlm.nih.gov/38075587/
Crissman Loomis is a former AI programmer, mathematician, health and longevity researcher, and the owner/operator of unaging.com
Timestamps: 0:00 Intro 1:08 5 Lifestyle Factors That Increase Life Expectancy To Around 90y 4:08 All-Cause Mortality (ACM) Data As A Guide To Potentially Get Beyond 90y 5:30 Incorporating Biomarkers Of Organ And Systemic Function For More Specificity 7:50 Optimizing Exercise Dosage 10:38 Using Biomarkers As A Strategy To Optimize Exercise Dose 12:00 Mike’s Exercise Specifics 16:05 Criss’s Exercise Dose 16:30 Titrating Exercise Dose 30:11 Mobility, Flexibility, Balance Training 35:35 Mobile Phenotype/Youthful Movement Pattern 39:25 Criss’s Diet 43:45 Is Calorie Restriction More Important Than Diet Composition? 54:45 Fasting 56:20 BMI Greater Than 25 Is Optimal Based On ACM Data? 1:00:30 Increased Lifespan With Fasting + CR + Circadian Alignment
1:09:30 Criss’s Marathon Training-Impact on CV Biomarkers?
Papers referenced in the video: Mortality rate and longevity of food-restricted exercising male rats: a reevaluation (Exercise increases average, but only CR increases average and maximal lifespan) https://pubmed.ncbi.nlm.nih.gov/9049716/
Female and male US Olympic athletes live 5 years longer than their general population counterparts: a study of 8124 former US Olympians https://pubmed.ncbi.nlm.nih.gov/32727712/
Resistance Training and Mortality Risk: A Systematic Review and Meta-Analysis (Lowest ACM risk for 75 minutes, but an increased ACM risk for greater than 170 minutes/week) https://pubmed.ncbi.nlm.nih.gov/35599175/
——————————————————————————————————————————-Papers referenced in the video:
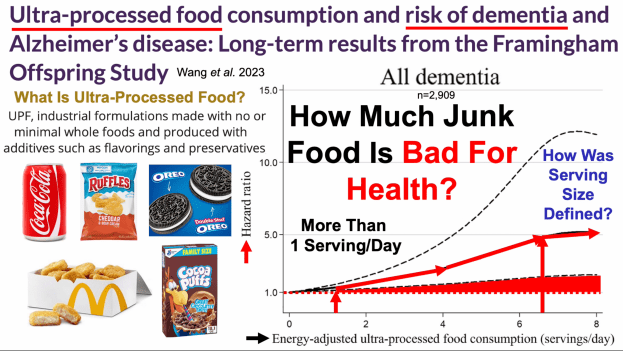
Ultra-processed food consumption and risk of dementia and Alzheimer’s disease: Long-term results from the Framingham Offspring Study https://pubmed.ncbi.nlm.nih.gov/37395366/
Dose–response meta-analysis of ultra-processed food with the risk of cardiovascular events and all-cause mortality: evidence from prospective cohort studies https://pubmed.ncbi.nlm.nih.gov/36866803/
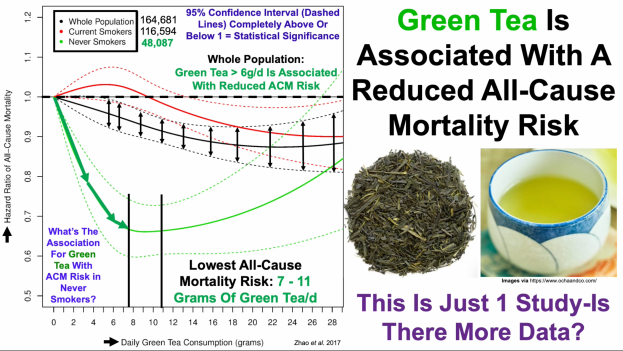
Papers referenced in the video: Green tea consumption and cause-specific mortality: Results from two prospective cohort studies in China https://pubmed.ncbi.nlm.nih.gov/28135196/
Green tea consumption and mortality in Japanese men and women: a pooled analysis of eight population-based cohort studies in Japan https://pubmed.ncbi.nlm.nih.gov/31392470/
Association between low-density lipoprotein cholesterol and cardiovascular mortality in statin non-users: a prospective cohort study in 14.9 million Korean adults https://pubmed.ncbi.nlm.nih.gov/35218344/
Increased red blood cell distribution width (RDW) is associated with higher glycosylated hemoglobin (HbA1c) in the elderly https://pubmed.ncbi.nlm.nih.gov/25651746/
Reduced oxidant stress and extended lifespan in mice exposed to a low glycotoxin diet: association with increased AGER1 expression https://pubmed.ncbi.nlm.nih.gov/17525257/
Gut microbiota drives age-related oxidative stress and mitochondrial damage in microglia via the metabolite N 6-carboxymethyllysine https://pubmed.ncbi.nlm.nih.gov/35241804/
Plasma Carboxymethyl-Lysine, an Advanced Glycation End Product, and All-Cause and Cardiovascular Disease Mortality in Older Community-Dwelling Adults https://pubmed.ncbi.nlm.nih.gov/19682127/
Advanced glycation end products and their circulating receptors predict cardiovascular disease mortality in older community dwelling women https://pubmed.ncbi.nlm.nih.gov/19448391/
Acute Hyperglycemia Causes Intracellular Formation of CML and Activation of ras, p42/44 MAPK, and Nuclear Factor KappaB in PBMCs https://pubmed.ncbi.nlm.nih.gov/12606501/
Experimental Hyperglycemia Alters Circulating Concentrations and Renal Clearance of Oxidative and Advanced Glycation End Products in Healthy Obese Humans https://pubmed.ncbi.nlm.nih.gov/30823632/
Novel associations between blood metabolites and kidney function among Bogalusa Heart Study and Multi-Ethnic Study of Atherosclerosis participants https://pubmed.ncbi.nlm.nih.gov/31720858/
Serum Carboxymethyl-lysine, a Dominant Advanced Glycation End Product, is Associated with Chronic Kidney Disease: the Baltimore Longitudinal Study of Aging https://pubmed.ncbi.nlm.nih.gov/19853477/