The main drawback to optimal health if you eat store-bought chocolate is that cacao beans are roasted, thereby increasing the concentration of the carcinogen, acrylamide (https://atomic-temporary-71218033.wpcomstaging.com/2014/07/27/acrylamide-is-in-chocolate-another-reason-why-cooking-food-at-high-temperature-is-not-good-for-you/). Besides eating homemade chocolate made from raw cacao beans (https://atomic-temporary-71218033.wpcomstaging.com/2014/09/21/homemade-chocolate-in-2-minutes/), are there any health benefits to drinking raw cacao?
The answer is yes, and it comes from the Kuna Indians, who live on a group of islands near Panama. The Kuna have been shown to have a low average blood pressure (BP, 110/70 mm Hg), and, do not experience the age-related increase in blood pressure that is common in Western society (Hollenberg et al. 1997). More importantly, death rates from cardiovascular disease and cancer, the #1 and #2 causes of death in the US were almost completely eliminated in the Kuna. Between 2000 to 2004, on the mainland of Panama, Bayard et al. (2007) reported that for every 100,000 residents, 83 died from cardiovascular disease (CVD), and 68 died from cancer. In contrast, per 100,000 Kuna, these death rates were reduced to 9 for CVD (a 9-fold reduction!) and 4 (a 15-fold reduction!) for cancer, respectively. In other words, cardiovascular disease and cancer are almost non-existent as a cause of death among the Kuna!
One could make the argument that the Kuna have decreased rates of CVD and cancer if it can be shown that their population is younger than on mainland Panama. The incidence of CVD and cancer increase with age, so if the Kuna population was younger than on the mainland, this could possibly explain their reduced death rates. However, the opposite was found to be true: approximately 94% of the residents of Panama are younger than 55 years of age, whereas ~87% of the Kuna are younger than 55. In addition, ~6% of Kuna’s population were found between the age of 55-64; ~4.4% were 65-74, and, ~2.4% were older than 75. In contrast, only 3% of mainland Panamanians were 55-64, ~1.9% were 65-74, and ~1.1% were older than 75 (Bayard et al. 2007). In other words, the percentage of Kuna older than 55 years was more than doubled, relative to mainland Panama! Not only do the Kuna have less CVD and cancer, they live longer than their mainland counterparts.
Before discussing how this is possible, it’s important to mention that the Kuna’s salt intake has been reported to be higher than both mainland Panama and, when compared with a Western diet. The Kuna eat, on average, 5500 mg of salt per day (Hollenberg et. al 1997). In comparison, Kuna who migrate to mainland Panama consume ~3300 mg/day (McCullough et. al 2006), subjects on a Western diet consume ~3700 mg, and, vegans consume ~1400 mg salt/day (Fontana et. al 2007). In other words, the Kuna eat more salt, but yet have lower BP, the absence of an age-related rise in BP, and have reduced risk of disease and mortality, relative to their Westernized-diet counterparts on the mainland of Panama.
Do the Kuna have genes that protect them from elevated blood pressure? If the Kuna were genetically protected, one would anticipate that they could move to an urban environment and maintain low blood pressure. However, Kuna that migrated to mainland Panama approximately 20 years earlier were found to have an increased incidence of both hypertension, and an age-related rise in BP (Hollenberg et. al 1997). This indicates that the Kuna were not protected by genes, and the factor that was keeping their blood pressure down was environmental.
So, how is this possible? There may be clues in the Kuna diet, which is almost exclusively plant and fish based, with almost no dairy, meat or nuts. The Kuna eat more fruit, 5 servings/day, vs. 1 serving/day on the mainland. The Kuna eat approximately 6 oz. fish/day, compared with, 1.5 oz/ day on the mainland (McCullough et. al 2006). Both increased fruit and fish intake may be responsible for the improved health that the Kuna experience, relative to their mainland counterparts.
But, there is another factor which is dramatically different in the Kuna diet when compared to the mainland-the Kuna consume more than 4 cups, or 30-40 ounces of a cocoa drink on a daily basis. Mainland Panamanians ingest little cocoa, and what they take is commercially available and flavanol-poor (McCullough et. al 2006). In contrast, unlike almost all commercially available chocolate, the cocoa consumed by the Kuna is not roasted. To make their cocoa drink, the Kuna grind raw cacao beans, which is then boiled with banana. After boiling this mixture, it is poured through a strainer, leaving behind the cocoa and banana solids. Because it’s not roasted, Kuna cocoa contains all of the health benefits of the cacao bean, with none of the acrylamide!
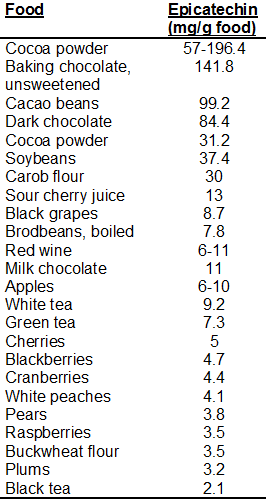
It’s important to note that the cocoa ingested by the Kuna is naturally very rich in a specific subclass of flavonoids known as flavanols, including epicatechin, catechin, and flavanol-based oligomers known as procyanidins (Chevaux et. al 2001, Fisher and Hollenberg 2005). Kuna cocoa beans provide 3000 mg/100g flavanols. Kuna cocoa powder provides less (flavanols are lost during the fermentation process), at ~2000 mg/100g cocoa. In contrast, 6 commercially available cocoa powders /cocoa drinks didn’t exceed 150 mg flavanols/100g cocoa (Fisher and Hollenberg 2005). High levels of flavanol have been shown to reduce risk of death from coronary artery disease by as much as 58% (Mukamal et al. 2002).
Since I don’t live with the Kuna off the mainland of Panama, I don’t have access to unfermented cacao beans. However, raw, organic, fermented, non-roasted cacao beans are indeed available online. To make the cocoa drink, I use 1 oz. of cacao beans, 1 medium-large banana and ~35 oz. of water, boiled for 10-15 minutes. Then, I pass this solution through a strainer, and drink it once it cools down. It’s delicious!
If you’re interested in watching an ABC news video on the Kuna and the preparation of this cocoa drink, here is the link:http://abcnews.go.com/Health/video/cocoa-kuna-indians-panama-native-americans-chocolate-production-13402637.

If you’re interested, please have a look at my book!
References:
Acrylamide data via: http://www.fda.gov/Food/FoodborneIllnessContaminants/ChemicalContaminants/ucm053549.htm
Bayard V, Chamorro F, Motta J, Hollenberg NK. Does flavanol intake influence mortality from nitric oxide-dependent processes? Ischemic heart disease, stroke, diabetes mellitus, and cancer in Panama. Int J Med Sci. 2007 Jan 27;4(1):53-8.
Chevaux KA, Jackson L, Villar ME, et al. Proximate mineral and procyandin content of certain foods and beverages consumed by Kuna Amerinds of Panama. J Food Composit Anal. 2001;14: 553–563.
Fisher NDL, Hollenberg NKH. Flavanols for cardiovascular health: the science behind the sweetness. J Hypertension. 2005;23: 1453–1459.
Fontana L, Meyer TE, Klein S, Holloszy JO. Long-term low-calorie low-protein vegan diet and endurance exercise are associated with low cardiometabolic risk. Rejuvenation Res. 2007 Jun;10(2):225-34.
Hollenberg NK, Martinez G, McCullough M, et al. Aging, acculturation, salt intake, and hypertension. Hypertension. 1997; 29:171–176.
McCullough ML, Chevaux K, Jackson L, Preston M, Martinez G, Schmitz HH, Coletti C, Campos H, Hollenberg NK. Hypertension, the Kuna, and the epidemiology of flavanols. J Cardiovasc Pharmacol. 2006;47 Suppl 2:S103-9; discussion 119-21.
Mukamal KJ, Maclure M, Muller JE, Sherwood JB, Mittleman MA. Tea consumption and mortality after acute myocardial infarction. Circulation 2002; 105:2476–2481.
http://www.nal.usda.gov/fnic/foodcomp/Data/Flav/Flav02-1.pdf