
High sensitivity C-Reactive Protein (CRP) is one of the 10 variables included in the biological age calculator, PhenoAge (https://michaellustgarten.wordpress.com/2019/09/09/quantifying-biological-age/). The reference range for CRP is 0 – 3 mg/L, but within that range, what’s optimal? To answer that question, it’s important to know how CRP changes during aging, and what levels are associated with an increased risk of death for all causes.
First, CRP increases 3-5 fold during aging in women and men, respectively (Ferrucci et al. 2005):

Investigating further, CRP continues to increase from relatively low levels of 0.7 mg/L (equivalent to 0.07 mg/dL) in 85-99 year olds to 2.5 mg/L (equivalent to 0.25 mg/dL) in adults older than 110y (Arai et al. 2015):

In support of this finding, the average CRP level in 98 centenarians (average age, 101y) was 5.4 mg/L, when compared with 3.2 mg/L in 70 year olds (Montoliu et al. 2014).
Based on the data for how CRP changes during aging, lower values would be expected to better in terms of risk of death for all causes. How low is optimal for CRP?
Several studies have investigated this issue. Risk of death for all causes was significantly reduced when CRP was < 3 mg/L, when compared with > 3 mg/L in the 11,193 subjects (average age 63y) of Oluleye et al. (2013). In terms of CRP values less than 3 mg/L, CRP < 1.0 mg/L was associated with significantly reduced risk of death for all causes in the 5,248 subjects (average age, 54y) of Hamer et al. (2010), in the 3,620 subjects (average age, 58y) of Koenig et al. (2008), in the 2,240 older adults (average age, 69y) of Elkind et al. (2009), and in the 1,519 subjects (average age 72y) of Kuoppamäki et al. (2015).
Similarly, CRP levels close to 1 mg/dL have also been associated with a significantly reduced risk of death for all causes, including < 0.86 mg/L in the 11,409 adults (average age, 59y) of Shen et al. (2019), and < 0.83 mg/L in the 1,476 men (average age, 53y) of Laaksonen et al. (2005).
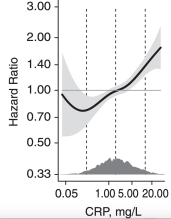
In terms of the association between CRP with risk of death for all causes, can we go lower than ~0.8 mg/L? CRP values < 0.5 mg/L were associated with reduced all-cause mortality risk, whereas values > 3 mg/L were associated with increased risk in the 16,850 non-smokers and non-users of hormone replacement therapy (average age, 58y) of Ahmadi-Abhari et al. (2013). Similarly, CRP between 0.5 – 1 mg/L, the area on the chart (see below) where the black line and the shaded 95% confidence interval have a hazard ratio < 1, was associated with a significantly reduced risk of death for all causes, whereas CRP > 5 mg/L was associated with an increased all-cause mortality risk in the 7,015 subjects of Zuo et al. (2016):
Going even lower, CRP < 0.33 mg/L (Tertile 1, white circle) was associated with a maximally reduced all-cause mortality risk when compared with values > 0.86 mg/L (Tertile 3, black circle) in the 1,034 older adults (average age, ~72y) of Shinkai et al. (2008):

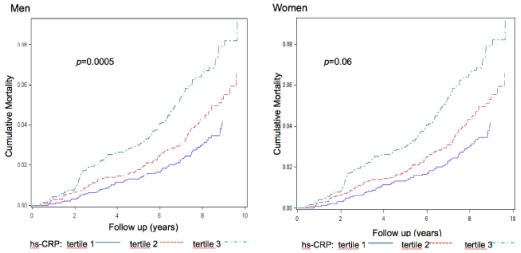
Similarly, CRP values between 0.03 – 0.33 mg/L in men and between 0.03 – 0.25 mg/L in women (blue lines for both men and women, Tertile 1) was associated with a significantly reduced risk of death for all causes in the 11,080 subjects (average age, 62y) of Nisa et al. (2016). In contrast, CRP > 0.85 mg/L in men and > 0.62 mg/L in women (close to significance in women, p=0.06; green lines for both, Tertile 3) was associated with an increased all-cause mortality risk:
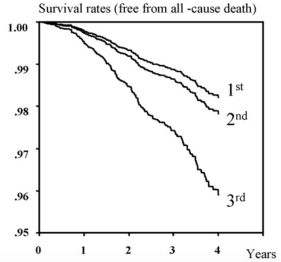
Lowest risk of death for all causes was also identified when CRP was between 0.1 – 0.3 mg/L (1st; Tertile 1), when compared with CRP > 0.8 mg/L (3rd; Tertile 3) in the 7,740 older adults (average age, 64y) of Makita et al. (2009):
Can we go lower than 0.3 mg/L for CRP and all-cause mortality risk? Yes! CRP < 0.21 mg/L was associated with a maximally reduced risk of death for all causes, and mortality risk significantly increased above 0.44 mg/L in the 2,589 subjects (average age, 59y) of Arima et al. (2008):

Collectively, based on these data, with the goal of optimal health and lifespan, I’d suggest that CRP levels should be as low as possible, and avoiding the age-related CRP increase. What are my CRP values? I’ve only measured it 6x, including once in 2009 (0.2 mg/L), once in 2018 (0.67 mg/L), and 4x in 2019 (0.41, 0.34, 0.47, 0.29 mg/L). My average value for 2019 is 0.38 mg/L, and I’d like to cut that in half. I have a blood test scheduled for next week, so stay tuned for that data!
Here’s the short version of this post in video format!
If you’re interested, please have a look at my book!
References
Ahmadi-Abhari S, Luben RN, Wareham NJ, Khaw KT. Seventeen year risk of all-cause and cause-specific mortality associated with C-reactive protein, fibrinogen and leukocyte count in men and women: the EPIC-Norfolk study. Eur J Epidemiol. 2013 Jul;28(7):541-50. doi: 10.1007/s10654-013-9819-6.
Arai Y, Martin-Ruiz CM, Takayama M, Abe Y, Takebayashi T, Koyasu S, Suematsu M, Hirose N, von Zglinicki T. Inflammation, But Not Telomere Length, Predicts Successful Ageing at Extreme Old Age: A Longitudinal Study of Semi-supercentenarians. EBioMedicine. 2015 Jul 29;2(10):1549-58. doi: 10.1016/j.ebiom.2015.07.029.
Arima H, Kubo M, Yonemoto K, Doi Y, Ninomiya T, Tanizaki Y, Hata J, Matsumura K, Iida M, Kiyohara Y. High–sensitivity C-reactive protein and coronary heart disease in a general population of Japanese: the Hisayama study. Arterioscler Thromb Vasc Biol. 2008 Jul;28(7):1385-91. doi: 10.1161/ATVBAHA.107.157164.
Elkind MS, Luna JM, Moon YP, Liu KM, Spitalnik SL, Paik MC, Sacco RL. High-sensitivity C-reactive protein predicts mortality but not stroke: the Northern Manhattan Study. Neurology. 2009 Oct 20;73(16):1300-7. doi: 10.1212/WNL.0b013e3181bd10bc.
Kuoppamäki M, Salminen M, Vahlberg T, Irjala K, Kivelä SL, Räihä I. High sensitive C-reactive protein (hsCRP), cardiovascular events and mortality in the aged: a prospective 9-year follow-up study. Arch Gerontol Geriatr. 2015 Jan-Feb;60(1):112-7. doi: 10.1016/j.archger.2014.10.002.
Ferrucci L, Corsi A, Lauretani F, Bandinelli S, Bartali B, Taub DD, Guralnik JM, Longo DL. The origins of age-related proinflammatory state. Blood. 2005 Mar 15;105(6):2294-9. Epub 2004 Nov 30.
Hamer M, Chida Y, Stamatakis E. Association of very highly elevated C-reactive protein concentration with cardiovascular events and all-cause mortality. Clin Chem. 2010 Jan;56(1):132-5. doi: 10.1373/clinchem.2009.130740.
Koenig W, Khuseyinova N, Baumert J, Meisinger C. Prospective study of high-sensitivity C-reactive protein as a determinant of mortality: results from the MONICA/KORA Augsburg Cohort Study, 1984-1998. Clin Chem. 2008 Feb;54(2):335-42.
Laaksonen DE, Niskanen L, Nyyssönen K, Punnonen K, Tuomainen TP, Salonen JT. C-reactive protein in the prediction of cardiovascular and overall mortality in middle-aged men: a population-based cohort study. Eur Heart J. 2005 Sep;26(17):1783-9.
Montoliu I, Scherer M, Beguelin F, DaSilva L, Mari D, Salvioli S, Martin FP, Capri M, Bucci L, Ostan R, Garagnani P, Monti D, Biagi E, Brigidi P, Kussmann M, Rezzi S, Franceschi C, Collino S. Serum profiling of healthy aging identifies phospho- and sphingolipid species as markers of human longevity. Aging (Albany NY). 2014 Jan;6(1):9-25.
Makita S, Nakamura M, Satoh K, Tanaka F, Onoda T, Kawamura K, Ohsawa M, Tanno K, Itai K, Sakata K, Okayama A, Terayama Y, Yoshida Y, Ogawa A. Serum C-reactive protein levels can be used to predict future ischemic stroke and mortality in Japanese men from the general population. Atherosclerosis. 2009 May;204(1):234-8. doi: 10.1016/j.atherosclerosis.2008.07.040.
Oluleye OW, Folsom AR, Nambi V, Lutsey PL, Ballantyne CM; ARIC Study Investigators. Troponin T, B-type natriuretic peptide, C-reactive protein, and cause-specific mortality. Ann Epidemiol. 2013 Feb;23(2):66-73. doi: 10.1016/j.annepidem.2012.11.004.
Nisa H, Hirata A, Kohno M, Kiyohara C, Ohnaka K. High-Sensitivity C-Reactive Protein and Risks of All-Cause and Cause-Specific Mortality in a Japanese Population. Asian Pac J Cancer Prev. 2016;17(5):2643-8.
Shen Y, Zhang Y, Xiong S, Zhu X, Ke C. High-sensitivity C-reactive protein and cystatin C independently and jointly predict all-cause mortality among the middle-aged and elderly Chinese population. Clin Biochem. 2019 Mar;65:7-14. doi:10.1016/j.clinbiochem.2018.12.012.
Shinkai S, Chaves PH, Fujiwara Y, Watanabe S, Shibata H, Yoshida H, Suzuki T. Beta2-microglobulin for risk stratification of total mortality in the elderly population: comparison with cystatin C and C-reactive protein. Arch Intern Med. 2008 Jan 28;168(2):200-6. doi: 10.1001/archinternmed.2007.64.
Zuo H, Ueland PM, Ulvik A, Eussen SJ, Vollset SE, Nygård O, Midttun Ø, Theofylaktopoulou D, Meyer K, Tell GS. Plasma Biomarkers of Inflammation, the Kynurenine Pathway, and Risks of All-Cause, Cancer, and Cardiovascular Disease Mortality: The Hordaland Health Study. Am J Epidemiol. 2016 Feb 15;183(4):249-58. doi: 10.1093/aje/kwv242.
