How much Vitamin C (ascorbic acid) is optimal for health? To answer this question, I’ll examine the association between circulating levels of Vitamin C with all-cause mortality risk. Then, which dietary Vitamin C intake corresponds to optimal plasma levels? Let’s have a look!
A variety of studies have investigated associations between plasma (or serum) Vitamin C with all-cause mortality risk:
- In a 4-year study of 1,115 older adults (average age ~79y), plasma vitamin C values greater than 66 uM (micromolar) were associated with significantly decreased all-cause mortality risk, when compared with values less than 17 uM (Fletcher et al. 2003).
- In a 12-year study of 725 older adults (average age, 73y), plasma vitamin C values greater than 52 uM were associated with significantly reduced all-cause mortality risk (Sahyoun et al. 1996). Interestingly, the most reduced mortality risk was found in those with plasma Vitamin C values greater than 89 uM, a value that can only be attained with dietary Vitamin C intakes greater than 1000 mg/day (more on this below!).
- In a 16-year study of 8,453 middle-aged adults (average age ~49y), serum Vitamin C values greater than 45 uM were associated with significantly reduced all-cause mortality risk, when compared with values less than 17 uM (Simon et al. 2001).
- In a 13-year study of 1,054 older adults (average age ~76y), elevated plasma levels of Vitamin C (risk ratios were reported without the actual Vitamin C concentration) were associated with significantly decreased all-cause mortality risk (Bates et al. 2011).
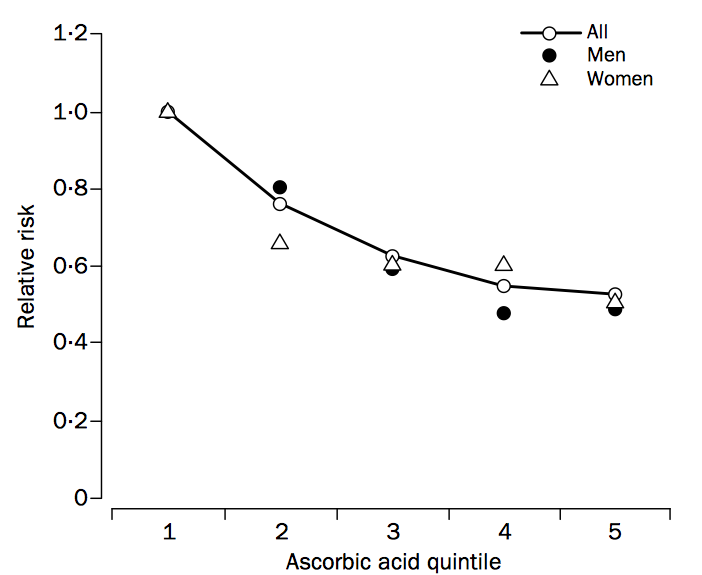
- In a 4-year study of 19,496 older adults (average age ~59y), plasma Vitamin C values greater than 48 uM in men and 59 uM in women (both in quintile 3, shown below) were associated with significantly reduced all-cause mortality risk (Khaw et al. 2001). The most reduced all-cause mortality risk included average Vitamin C values of 73 uM for men and 85 uM for women (shown below in quintile 5), values which require greater than 500 mg of dietary Vitamin C/day (more on this also below!).
Studies that show weaker or no association between the plasma Vitamin C concentration with all-cause mortality risk include Loria et al. (2000) and Jia et al. (2007). In Loria et al. (2000), 9,450 middle aged adults (~48y) were followed for 12-16 years. Men in the highest Vitamin C quartile (> 74 uM) had significantly reduced all-cause mortality risk, when compared with men in the low plasma Vitamin C group (< 28 uM). Although a similar association was identified for women, significance was lost after multivariable adjustment. In Jia et al. (2007), although plasma Vitamin C values less than 61 uM were associated with increased all-cause mortality risk in older adults (median age, ~80y) that were studied for ~7.5 years, these data were not statistically significant (p-value = 0.18). However, the study sample size (398 subjects) may have been too small to detect significant effects.
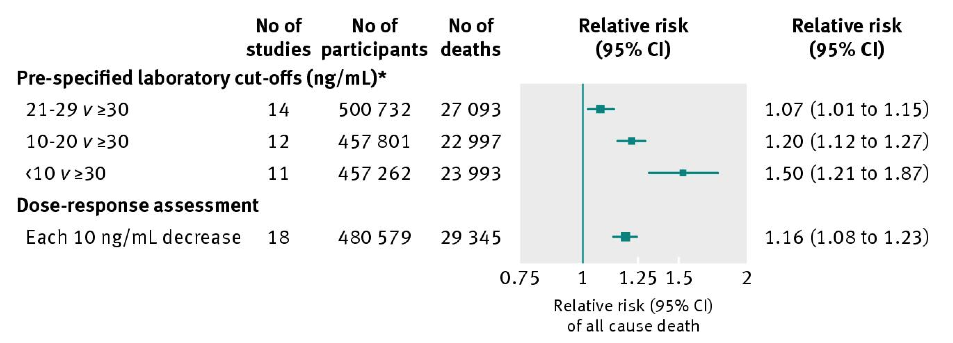
Collectively these studies show that low circulating levels of Vitamin C may be related to increased mortality risk, whereas plasma values greater than ~50 uM are consistently associated with reduced all-cause mortality risk. How much dietary vitamin C is required to attain 50 uM+?
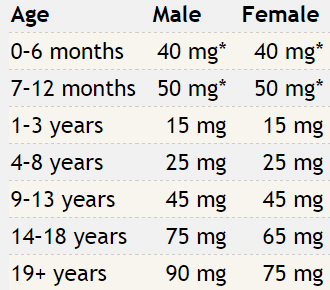
As shown below, the RDA for dietary Vitamin C is 90 mg for males and 75 mg for females older than 19 years (Institute of Medicine 2000).
If you consume the RDA for Vitamin C, what plasma Vitamin C concentration will that yield? Shown below is how the plasma Vitamin C concentration varies according to ingested dose (Levine et al. 1996). Consuming the RDA value for Vitamin C yields a plasma Vitamin C value of 20-30 uM. From the studies listed above, that would put you in the increased all-cause mortality risk group! How much dietary Vitamin C would be needed to achieve plasma values greater than 50 uM? From the plot, we see that a dietary Vitamin C intake at double the RDA would be necessary. Furthermore, because 2 studies have reported decreased all-cause mortality risk at plasma Vitamin C values greater than 66 uM, dietary intakes intake between 500-1000+ mg/day may be necessary:

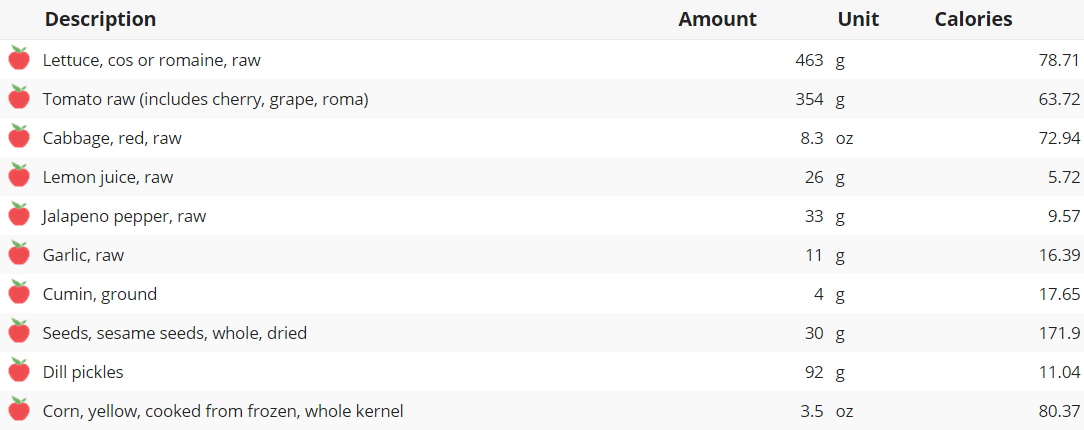
Which foods are Vitamin C-rich? As shown below, sweet peppers (yellow, red, and green) are the All-Stars for Vitamin C content per 100 calories:

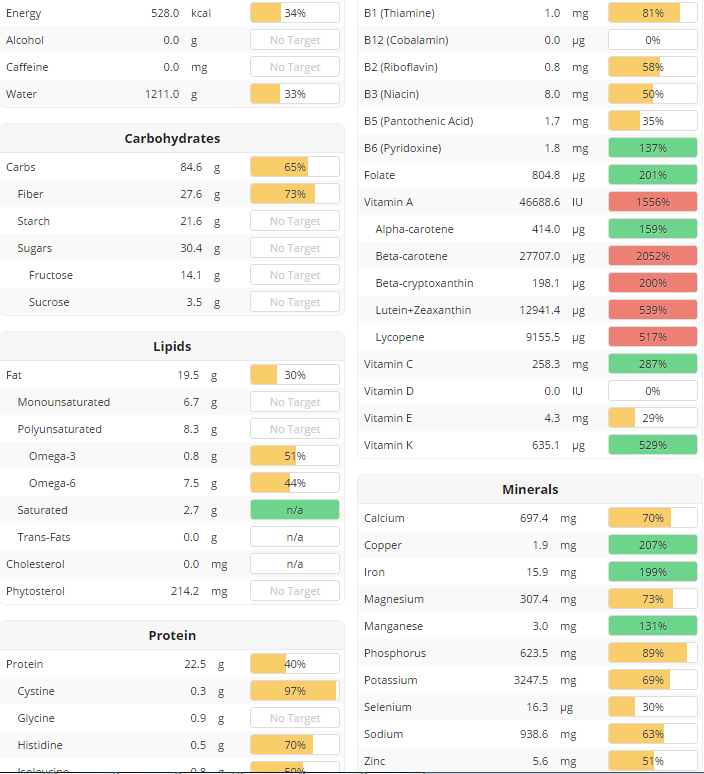
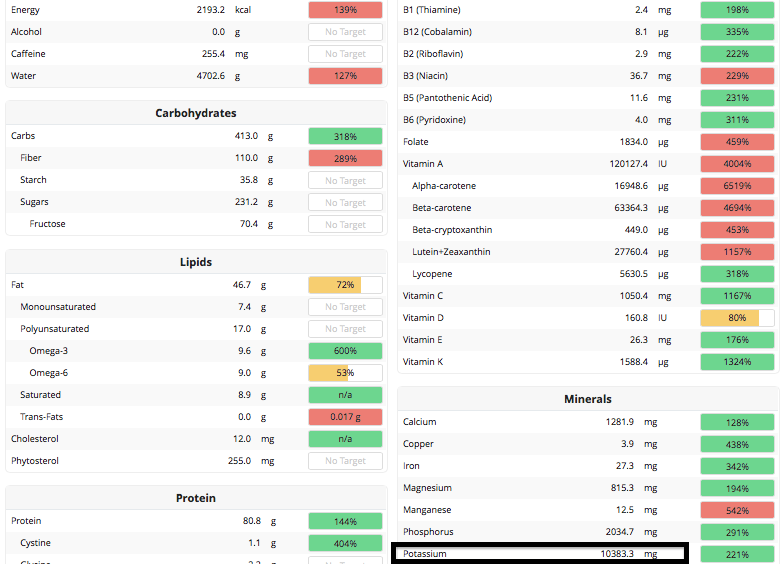
What’s my average daily Vitamin C intake? Shown below is my average daily Vitamin C intake, 875 mg/day, separated by month. Based on that value, my plasma Vitamin C concentration should be ~ 70 uM, which may be associated with maximally reduced all-cause mortality risk.

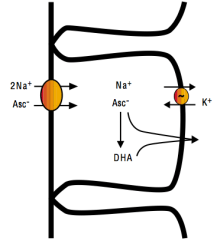
With the goal of optimizing plasma Vitamin C, it is also important to monitor dietary sodium intake. Intestinal absorption of Vitamin C requires dietary sodium (Friedman and Zeidel 1999). As shown below, 1 ascorbate ion (asc-) is absorbed from the intestinal lumen into intestinal epithelial cells in the presence of 2 sodium (Na+) ions. Vitamin C can then diffuse into the blood as Asc- or as dehydroascorbate (DHA):
Accordingly, based on my average dietary Vitamin C intake of 875 mg/day, to maximize absorption, a corresponding dietary sodium intake of 1750 mg would also be necessary.
If you’re interested, please have a look at my book!
References
Bates CJ, Hamer M, Mishra GD. Redox-modulatory vitamins and minerals that prospectively predict mortality in older British people:the National Diet and Nutrition Survey of people aged 65 years and over. Br J Nutr. 2011 Jan;105(1):123-32.
Fletcher AE, Breeze E, Shetty PS. Antioxidant vitamins and mortality in older persons: findings from the nutrition add-on study to the Medical Research Council Trial of Assessment and Management of Older People in the Community. Am J Clin Nutr. 2003 Nov;78(5):999-1010.
Friedman PA, Zeidel ML. Victory at C. Nat Med. 1999 Jun;5(6):620-1.
Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. Washington, DC: National Academy Press, 2000.
Jia X, Aucott LS, McNeill G. Nutritional status and subsequent all-cause mortality in men and women aged 75 years or over living in the community. Br J Nutr. 2007 Sep;98(3):593-9.
Khaw KT, Bingham S, Welch A, Luben R, Wareham N, Oakes S, Day N. Relation between plasma ascorbic acid and mortality in men and women in EPIC-Norfolk prospective study: a prospective population study. European Prospective Investigation into Cancer and Nutrition. Lancet. 2001 Mar 3;357(9257):657-63.
Levine M, Conry-Cantilena C, Wang Y, Welch RW, Washko PW, Dhariwal KR, Park JB, Lazarev A, Graumlich JF, King J, Cantilena LR. Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. Proc Natl Acad Sci U S A. 1996 Apr 16;93(8):3704-9.
Loria CM, Klag MJ, Caulfield LE, Whelton PK. Vitamin C status and mortality in US adults. Am J Clin Nutr. 2000 Jul;72(1):139-45.
Sahyoun NR, Jacques PF, Russell RM. Carotenoids, vitamins C and E, and mortality in an elderly population. Am J Epidemiol. 1996 Sep 1;144(5):501-11.
Simon JA, Hudes ES, Tice JA. Relation of serum ascorbic acid to mortality among US adults. J Am Coll Nutr. 2001 Jun;20(3):255-63.