In the first 45 minutes, discuss each of the biomarkers contained within Levine’s Biological Age calculator, Phenotypic Age.
After that, I answer questions from the audience and we discuss all things related to aging.
In the first 45 minutes, discuss each of the biomarkers contained within Levine’s Biological Age calculator, Phenotypic Age.
After that, I answer questions from the audience and we discuss all things related to aging.

Here’s a recent podcast that was recorded with Julian Hayes II at Optimal Health for Busy Entrepreneurs:
https://theartoffitnessandlife.com/episode20/
Enjoy!
CD8+ T cells are a subset of lymphocytes that play a major role in antiviral defense (Kulinski et al. 2013). However, recently published evidence shows reduced levels of circulating CD8+ T cells in people infected with SARS-CoV-2 (Zheng et al. 2020, Wang et al. 2020; HC= healthy controls, NCP = patients with COVID-19 related pneumonia):

Immune enhancing treatments, including thymalfasin and immunoglobulin are being provided to SARS-COV-2 infected subjects with some success. For example, 37/55 (67%) subjects saw improvements for circulating CD8+ levels in Wang et al. 2020, but additionally, 18/55 subjects did not experience increased CD8+ counts:

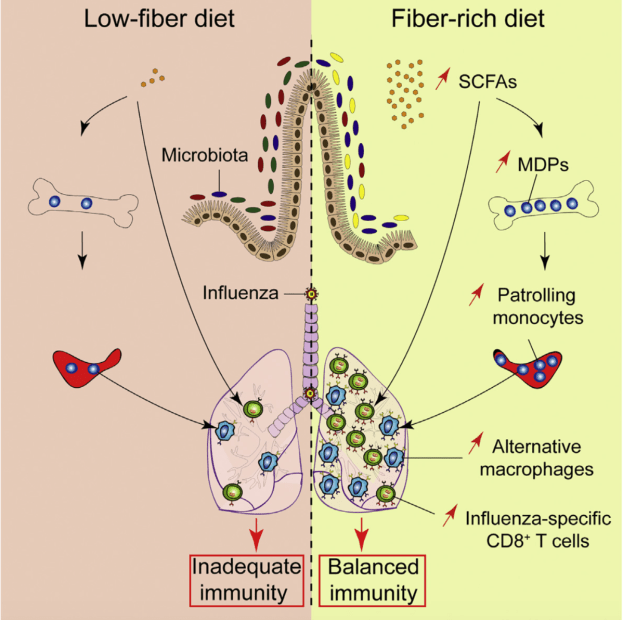
Accordingly, levels of CD8+ T cells were identified as an independent predictor for COVID-19 severity and treatment efficacy (Wang et al. 2020). When considering that CD8+ cells were not increased in all subjects in Wang et al., are there are other strategies that may be helpful? Interestingly, increased levels of CD8+ cells are found in the lungs of mice infected with the influenza A virus in response to a high soluble-fiber diet, when compared with control-fed mice (Trompette et al. 2018):

As a result, lung viral load is more than 10-times reduced 8-days after infection in high soluble fiber-fed mice:

Moreover, average survival in mice infected with influenza A is significantly better when fed the high soluble-fiber diet, when compared with control fed-mice:

Is it possible that a high soluble fiber diet can increase CD8+ cells in people infected with SARS-CoV-2, thereby enhancing their recovery and survival? No studies have tested this hypothesis (yet). While conventional medical treatment is obviously helpful, based on the findings of Trompette et al. (2018), further optimization of immune defense against viral infections may occur when including soluble fiber-rich foods.
References
Kulinski JM, Tarakanova VL, Verbsky J. Regulation of antiviral CD8 T-cell responses. Crit Rev Immunol. 2013;33(6):477-88. Review.
Trompette A, Gollwitzer ES, Pattaroni C, Lopez-Mejia IC, Riva E, Pernot J, Ubags N, Fajas L, Nicod LP, Marsland BJ. Dietary Fiber Confers Protection against Flu by Shaping Ly6c– Patrolling Monocyte Hematopoiesis and CD8+ T Cell Metabolism. Immunity. 2018 May 15;48(5):992-1005.e8. doi: 10.1016/j.immuni.2018.04.022.
Wang F, Nie J, Wang H, Zhao Q, Xiong Y, Deng L, Song S, Ma Z, Mo P, Zhang Y. Characteristics of peripheral lymphocyte subset alteration in COVID-19 pneumonia. J Infect Dis. 2020 Mar 30. pii: jiaa150. doi: 10.1093/infdis/jiaa150.
Zheng M, Gao Y, Wang G, Song G, Liu S, Sun D, Xu Y, Tian Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020 Mar 19. doi: 10.1038/s41423-020-0402-2.
Coronavirus isn’t the only virus that negatively affects human health.
For more info,
https://www.amazon.com/dp/B01G48A88A
There are a few ways that we can fight the novel coronavirus (SARS-CoV-2). Clinical trials aimed at vaccination have recently begun, and at the earliest, could be available within 6-18 months. Similarly, drugs aimed at inhibiting, blocking, or reducing viral replication, including remdesevir and hydoxychloroquine are entering clinical trials, but large-scale results are also a few months away.
Other alternatives that are rarely discussed are dietary components that can inhibit SARS-CoV-2 replication. Inhibiting replication is important because if the virus continually makes more copies of itself, there will be a systemic viral overload, thereby overwhelming the immune system. Two coronavirus proteins that are important for its replication and binding to cell membranes are its Main protease (Mpro for SARS-CoV-2, 3CLpro for SARS-CoV; X. Liu & Wang, 2020), and its surface Spike glycoprotein (S protein; Song et al. 2018), respectively.
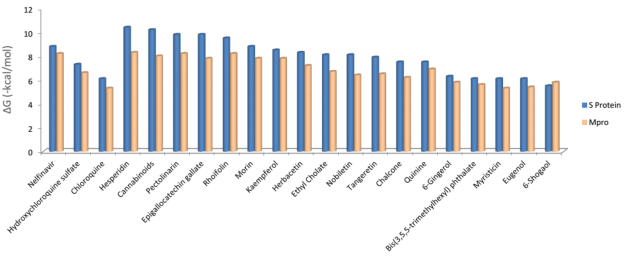
In a recently published (but not peer-reviewed) preprint, Tallei et al. (2020) used a molecular docking approach to predict how SARS-CoV-2’s Mpro and S proteins interact with various drugs and plant-based compounds. A lower molecular docking value is indicative of a potentially better ability to inhibit these proteins. Interestingly, many plant-based metabolites have lower (or equal) molecular docking values when compared with coronavirus-based drugs:
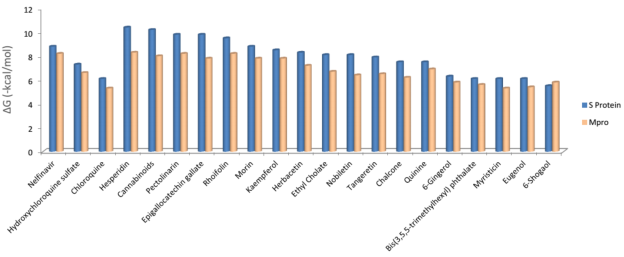
For example, when compared with the drugs nelfinavir, hyrdroxychloroquine sulfate, and chloroquine, hesperidin (found in citrus fruits and peppermint) and epigallocatechin galleate (found in green tea, apple skin, plums, onions, hazelnut) had equivalent or lower molecular docking scores, evidence that suggests a better ability for the plant-based metabolites to inhibit Mpro and the S protein. Based on this data, incorporation of these foods may be an important strategy for boosting endogenous defense against SARS-CoV-2 infection.
Similarly, a molecular docking approach was used to identify potential inhibitors for Mpro in another recent preprint (Khaerunnisa et al. 2020). When compared with the docking energy for Mpro’s native ligand (-8), the coronavirus drugs nelfinavir and lopinavir had lower docking energies, thereby suggesting that they would be good Mpro inhibitors. Interestingly, kaempferol and quercetin had docking energies that were not as low as the drugs, but were as low as or lower than the docking energy for Mpro’s native ligand, thereby suggesting that they might also act as inhibitors of SARS-CoV-2 replication:
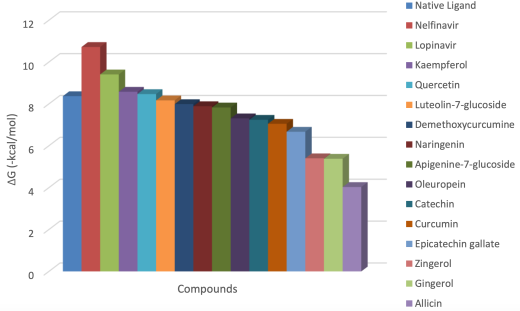
Kaempferol and quercetin are found in relatively high amounts in dill, lettuce, onions, spinach and other vegetables (for the full list see https://www.ars.usda.gov/ARSUserFiles/80400525/Data/Flav/Flav_R03.pdf).
It’s important to note that the amount of these foods needed to ingest enough kaempferol, quercetin, or other metabolites that may inhibit SARS-CoV-2 replication or its fusion to cell membranes proteins in vivo is unknown. In addition, with the goal of further boosting endogenous defense, I’d propose including these foods in addition to, but not for the replacement of a vaccine or FDA approved medicines. Note that clinical trials aimed at direct testing for the ability of these plant-based components to inhibit SARS-CoV-2 replication has yet to be performed, but when consumed as a part of a whole-food diet, may be a low risk, high reward strategy for battling SARS-CoV-2 infection.
References
Khaerunnisa, S., Kurniawan, H., Awaluddin R., Suhartati S., Soetjipto, S. (2020). Potential Inhibitor of COVID-19 Main Protease (Mpro) from Several Medicinal Plant Compounds by Molecular Docking Study. March 13, Preprint. doi: 10.20944/preprints202003.0226.v1
Liu, X., & Wang, X.-J. (2020). Potential inhibitors for 2019-nCoV coronavirus M protease from clinically approved medicines. BioRxiv, 2020.01.29.924100. https://doi.org/10.1101/2020.01.29.924100.
Song, W., Gui, M., Wang, X., & Xiang, Y. (2018). Cryo-EM structure of the SARS coronavirus spike glycoprotein in complex with its host cell receptor ACE2. PLOS Pathogens, 14(8), e1007236. https://doi.org/10.1371/journal.ppat.1007236.
Tallei, T.E., Tumilaar, S.G., Niode, N.J. , Fatimawali, Kepel4, B.J., Idroes, R., Effendi Y. (2020). Potential of Plant Bioactive Compounds as SARS-CoV-2 Main Protease (Mpro) and Spike (S) Glycoprotein Inhibitors: A Molecular Docking Study. April 9, Preprint. doi: 10.20944/preprints202004.0102.v2.
Coronavirus isn’t the only virus that negatively affects human health. For more info,
https://www.amazon.com/dp/B01G48A88A
Exactly 1 month ago, my first biological age measurement of 2020 was 32.75y (https://michaellustgarten.wordpress.com/2020/02/14/biological-age-32-75y-chronological-age-47y-first-2020-measurement/). When considering that my chronological age is 47y, that’s a 14 year improvement, but I wasn’t (and still aren’t) satisfied. When I sent my blood for analysis, I was battling a mild upper respiratory infection (cough, no fever), which likely raised my WBCs, thereby resulting in a higher biologic age. Also, I was experimenting with a higher intake of meat, eggs, and cheese, to see what affect that it would have on my circulating biomarkers. On that blood test in February, my creatinine levels were higher than my 2015-2020 average value, and if those foods were associated with circulating levels of creatinine, reducing them should also reduce creatinine, and accordingly, further improve my biological age. I also assumed that all other variables on Levine’s Phenotypic Age calculator would be unchanged.
On March 9 2020, I sent my blood for analysis so that I could calculate biological age with Levine’s PhenotypicAge. Almost exactly as expected, my WBCs (4.7 * 10^3 cells/microliter) were closer to my 2015-2020 average value (4.6), rather than the higher value (5.8) in my blood test last month. Similarly, reducing my intake of beef, eggs, and cheese brought creatinine from 1.08 to 0.97 mg/dL, which is closer to its 5-year average (0.94 mg/dL). As a result, I further reduced my biological age by 1.14 years to 31.61y, which is 15+ years younger than my chronological!

Because I track my diet every day, I can investigate the correlation between my meat, eggs, and cheese intake with creatinine. I now have 8 blood tests that correspond to dietary data, and interestingly, there is a moderately strong correlation between my average daily beef+egg+cheese intake with creatinine (r = 0.55). Based on these data, I’m going to continue to minimize consumption of these foods, with the goal of optimizing creatinine.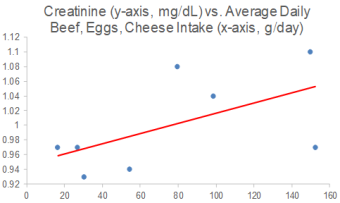
On a final note, I also expected to further reduce my CRP from 0.3 to something lower, but it slightly increased to 0.37 mg/L. While that is far from a high value, lower is better, and in future blood tests I’ll try to figure out how to further reduce it.
If you’re interested in calculating your biological age, here’s the Excel link:
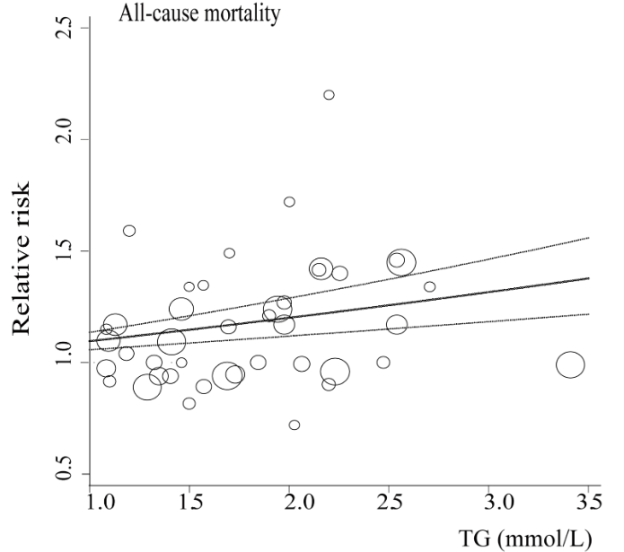
In terms of all-cause mortality risk, is the reference range for circulating triglycerides (TG, <150 mg/dL) optimal?
A meta-analysis of 38 studies in 360,556 subjects with a median age of 48y and a 12-year follow-up reported lowest all-cause mortality risk for subjects with TG values less than 90 mg/dL (equivalent to ~1 mmol; Liu et al. 2013). As shown below, each successive 90 mg/dL increase was associated with a 12% higher all-cause mortality risk. A person with a value closer to the high end of the reference range, ~150 would have a ~7% increased mortality risk compared someone with a value ~90. In other words, there would be 7 more deaths per 100 total people at a TG value of 150, compared with the death rate for people with values less than 90.

Added importance for the association between TG values less than 90 with all-cause mortality risk come from studies of people who have lived longer than 100 years, centenarians. As shown below, triglyceride values less than 101 mg/dL have been reported in 9 of 11 centenarian studies:

What’s my TG value? As shown below, I’ve measured triglycerides 23 times since 2015, with an average value of 52 mg/dL:
With the goal of keeping triglyceride levels low, are there dietary factors that influence it? When compared with my dietary data, the strongest correlation (r = 0.73, R2=0.5339) is present for triglycerides with my calorie intake. In other words, a higher daily calorie intake is associated with higher levels of triglycerides:

Based on this correlation, should my triglycerides start to rise in the future, a first step would be reducing my average daily calorie intake, which since October 2019 has been ~2550 calories/day.
If you’re interested, please have a look at my book!
References
Liu J, Zeng FF, Liu ZM, Zhang CX, Ling WH, Chen YM. Effects of blood triglycerides on cardiovascular and all-cause mortality: a systematic review and meta-analysis of 61 prospective studies. Lipids Health Dis. 2013 Oct 29;12:159.

Measurement of biological age with Levine’s Phenotypic Age calculator is strongly correlated with chronological age (r=0.94; see https://michaellustgarten.wordpress.com/2019/09/09/quantifying-biological-age/). In 2019, I measured all 9 of its analytes 3 times, with biological age readings of 35.39y, 35.58y, and 31.3y, for an average 2019 biological age of 34.09y (see https://michaellustgarten.wordpress.com/2019/11/01/biological-age-31-3y-chronological-age-46y/). That’s 12 years younger than my chronological age in 2019, 46y!
On Feb 12, I had my first blood test measurement of 2020. I expected to see a worse biological age, as over the past week, I’d been hit with the flu, and since my last measurement in 2019, I made a few changes to my diet that I didn’t expect to favorably affect it. In contrast, I’ve been purposefully in a mild caloric restriction in an attempt to reduce my body fat from a relatively lean 10-12% to lower values. Since my last blood test 3+ months ago, my average calorie intake was 2553, which is 5-10% less than my maintenance intake, 2700-2800 calories/day. So how did these variables affect my biologic age? Let’s have a look at the data!

My biological age was 32.75y, which is less than my 2019 average value, and better than I expected considering the factors mentioned above! Note that there is room for improvement, including my creatinine and WBC levels, which both increased when compared with my average 2015-2019 values (which included 23 blood tests). My average daily fiber intake has been ~100g/day for a few years, and over the past 3 months, I purposefully reduced that to ~70g/day. Conversely, I increased my intake of meat, eggs, and cheese intake during that period, to see if eating less fiber and more animal products would negatively impact my blood test results. For me, eating more animal protein and less total fiber may not be optimal, as my creatinine levels also rose in 2019 when I performed a similar dietary experiment. Note that creatinine levels increase with age (see https://michaellustgarten.wordpress.com/2019/11/18/optimizing-biologic-age-creatinine/), so if I can avoid that by altering my diet, I will. For the next blood test, I’ll reduce, but not eliminate my intake of meat, eggs, and cheese, and I expect that my creatinine levels will decrease back towards my average 2015-2019 value of 0.94 mg/dL.
Also note my WBCs-although they’re not higher than the 3.5-6 optimal range (see https://michaellustgarten.wordpress.com/2019/10/11/blood-testing-whats-optimal-for-wbc-levels/), they’re increased when compared with my average 2015-2019 value of 4.5. This increase is more than likely a result of the flu/infection that I’m battling. Once it passes, I expect it to return to close to my average WBC value, ~4.5.
Going forward, I expect my creatinine and WBCs to come down to their average values, which would result in a biological age that is closer to 30y on my next blood test. Stay tuned for that data!
To quantify your biological age using Levine’s Phenotypic Age calculator, here’s the Excel link! DNAmPhenoAge_gen (1)
If you’re interested, please have a look at my book!

How’s my progress on the road to achieving a resting heart rate (RHR) as close to 40 beats per minute (bpm) as possible? Shown below is my RHR data for August 2018-Jan 2019, which corresponds to the 6-month period after I started tracking RHR. When compared with that period, am I still making year-over-year progress?
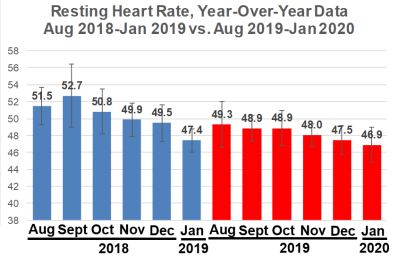
First, note that my Jan 2019 RHR value of 47.4 bpm seems dramatically reduced when compared with Aug-Dec 2018. My computer crashed in Jan 2019, and I lost 4 days of January 2019 RHR data, with remaining data for 27 days. Accordingly, I didn’t expect to be better than that, year-over-year. Nonetheless, my average RHR for Jan 2020 is 46.9 bpm, which is superficially better, but it isn’t statistically different from Jan 2019 (p = 0.13). However, my RHR is still going in the right direction!
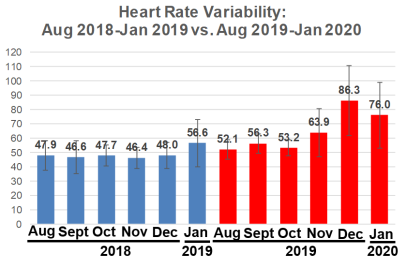
What about my heart rate variability (HRV)? Relative to Jan 2019 (56.6), my HRV in Jan 2020 was significantly higher (76; p=0.003), but note that I didn’t additionally improve my HRV relative to December 2019 (86.3).
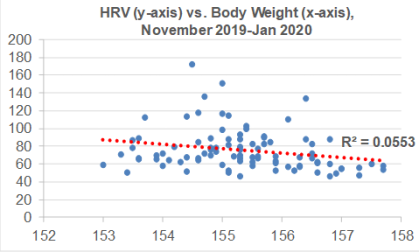
I’ve been consistent with my exercise program, including weekly workouts (3-4x, ~1 hr each session) and walking (15-20 miles), so are there other variables that may explain the sudden increase in HRV from Nov 2019-Jan 2020? During that time, I’ve been cutting my calorie intake by a small amount (~100-200 cals/day) below my body weight maintenance intake, with the goal of getting leaner. As a result, I’ve slowly decreased my body weight from 157 to 154 during that time. Although there is a weak negative correlation between my body weight with HRV (R2=0.0553), this association is statistically significant (p=0.024). So reducing body weight may have played a role in the sudden HRV increase:
For those who may have missed my other post updates for RHR and/or HRV:
Dec 2019 update: https://michaellustgarten.wordpress.com/2020/01/01/resting-heart-rate-heart-rate-variability-december-2019-update/
Oct, Nov 2019 update: https://michaellustgarten.wordpress.com/2019/12/05/resting-heart-rate-heart-rate-variability-still-making-progress/
Sept 2019 update: https://michaellustgarten.wordpress.com/2019/10/08/resting-heart-rate-year-over-year-update/
Also, why a RHR as close to 40 bpm may be optimal: https://michaellustgarten.wordpress.com/2019/02/02/resting-heart-rate-whats-optimal/
If you’re interested, please have a look at my book!
A meta-analysis of 10 studies, including 80,139 subjects was recently published that shows a significantly reduced risk of death for all causes in association with higher total dietary fiber intakes (35-39g/day), when compared with lower fiber (Reynolds et al. 2019):

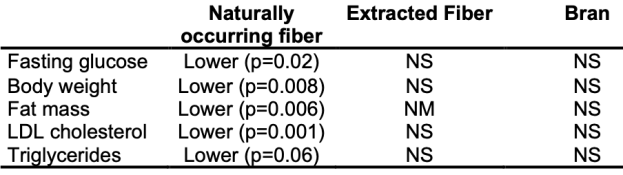
Should we supplement with fiber, or get it from whole food? Fiber from whole foods was significantly associated with lower levels of fasting glucose, body weight, whole body fat mass, LDL cholesterol, and triglycerides. Supplementation with fiber extracts or bran was not significantly associated with the reduction of any of these variables (NS, not significant; NM, not measured:

Reference
Reynolds A, Mann J, Cummings J, Winter N, Mete E, Te Morenga L. Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet. 2019 Feb 2;393(10170):434-445. doi: 10.1016/S0140-6736(18)31809-9.
If you’re interested, please have a look a my book!
